
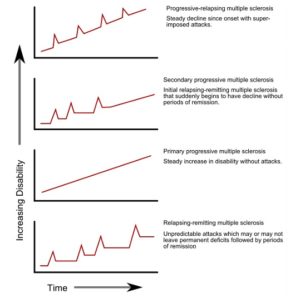
Multiple sclerosis (MS) was first described by Charcot in 1868. The hallmark of MS is the multiple episodes of Central Nervous System (CNS) affliction at different times (Dissemination in time and space). CNS includes the brain, spinal cord and optic nerves. Often some may be silent (asymptomatic). This is the most common (85%) type and is called Relapsing Remitting MS (RMMS) because relapses occur with remission often being incomplete. The other 15% have a progressive course from the onset and are called Primary Progressive MS (PPMS). However, a large majority of those with RRMS will a decade or three later have a progressive decline and these are categorised as Secondary Progressive MS (SPMS).
Fig 1:- Progression of MS subtypes- Source: Wikipedia
It has been long held that MS is an inflammatory condition in which an inflammatory reaction is set off and enters through the blood-brain barrier (BBB) to attack the myelin (The insulation that coats all axons arising from neurons (brain cells). Thus, this has been characterised as primarily a white matter disease (Axonal atrophy) as opposed to grey matter or neurons. Thus grey matter is thought to be a secondary bystander. The earlier hypothesis is also called the ’inside-out’ phenomenon. Management of MS has almost totally focussed on reducing the inflammation with immuno-modulators like steroids, IgG, interferon etc. This is given at the time of each relapse of RRMS and is therefore symptomatic and not curative. In fact, there is no cure for MS. In SPMS and PPMS there is little to offer as these are primarily degenerative.
This concept has in recent times come under attack as in the progressive forms (both PPM and SPMS) no inflammation is seen and in fact neurodegeneration is seen. Both forms ultimately have the same downward clinical course. Also, pathophysiologically they are identical. Further, degeneration can and does occur in the absence of inflammation. They could thus be parallel processes. Some have hypothesised that degeneration could be the trigger that invites inflammation – the ‘inside – out’ concept. There is evidence for this as halting the inflammation does not reduce or halt the degeneration. Grey matter atrophy is seen is most MS especially the progressive types. Even in ‘normal’ grey matter of MS patients on histochemistry abnormalities are seen. Mitochondrial dysfunction is thought to be at the heart of this. Mitochondria are the power-houses of the cells and energy depletion due to its malfunctioning can lead to axonal atrophy and neuronal loss. Such mitochondrial injury is seen in experimental autoimmune encephalomyelitis (EAE). Targeting this dysfunction could be an important therapeutic tool. COQ10 and ubiquinone have been tried in clinical and experimental milieu with variable results.
Therapeutic targets would theoretically include:-
1. Glucose hypometabolism
2. Reduction in reactive oxygen species (ROS)
3. Mitochondrial biogenesis
4. Anti-inflammatory
5. Increase in ATP
6. Neuroprotection
All these can be achieved by a ketogenic diet (KD)
For detailed case study on Ketogenic diet in Multiple sclerosis patient please view our NEWS page.